SURGERY I
UNIT 4: SHOCK
CTEVT Health Science Second Year | Syllabus 2024
🚨 Quick Navigation – Types of Shock
⚠️ Introduction to Shock
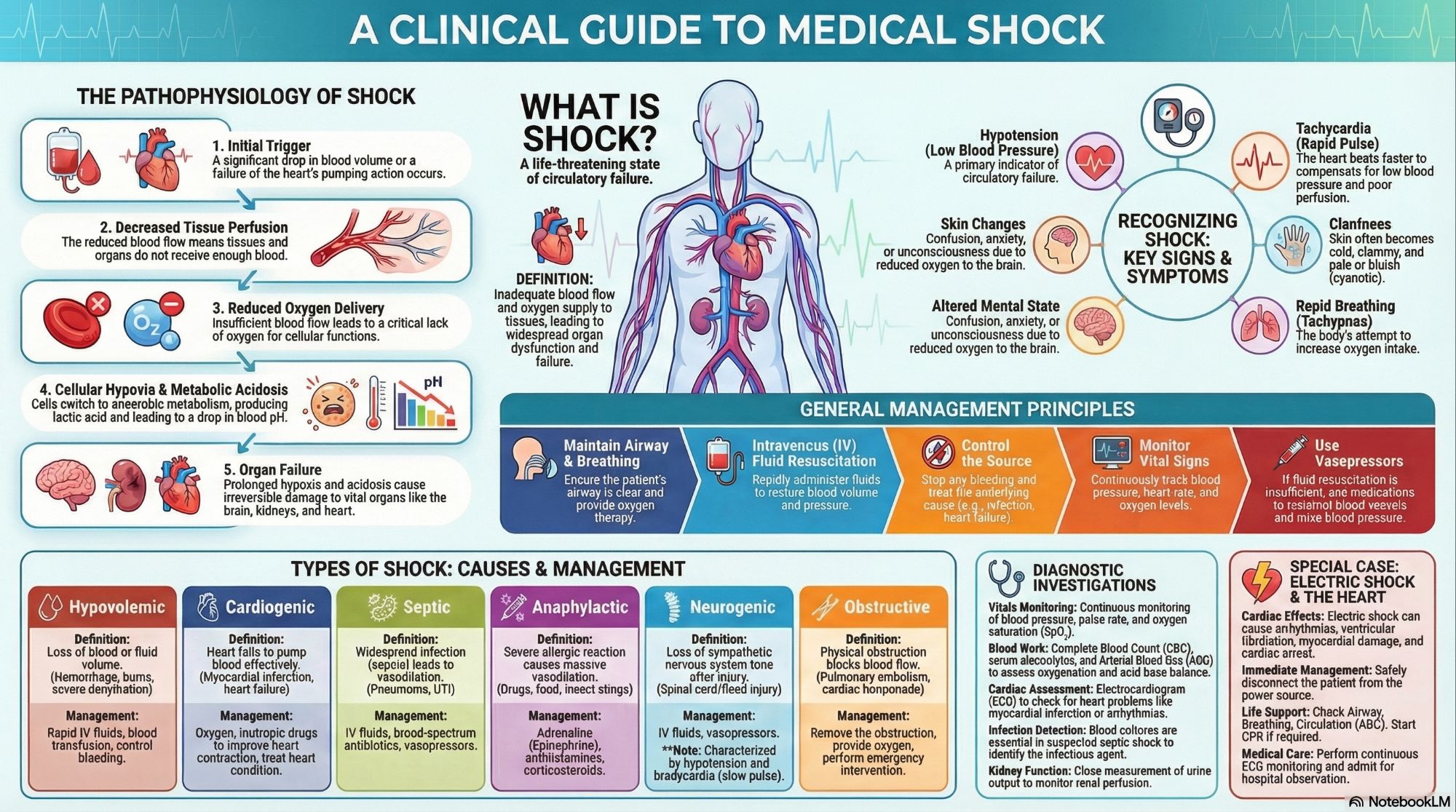
Shock is a life‑threatening condition characterized by inadequate tissue perfusion and oxygen delivery, leading to cellular hypoxia, metabolic acidosis, and eventual organ failure. It is a medical emergency requiring immediate recognition and intervention.
📋 Definition of Shock
“A state of cellular and tissue hypoxia due to reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen utilization.”
This leads to anaerobic metabolism, lactic acidosis, and end‑organ dysfunction if not promptly reversed.
🔄 Pathophysiology of Shock
Initiating Event
Blood loss, MI, infection, allergy, etc.
↓ Tissue Perfusion
Reduced oxygen delivery
Cellular Hypoxia
Anaerobic metabolism
Organ Failure
Brain, kidney, heart, lungs
🎯 Key Pathophysiological Concepts
↓ Preload: Reduced venous return
↓ Contractility: Impaired heart pump function
↑ Afterload: Increased systemic vascular resistance
Microcirculatory dysfunction: Impaired capillary flow
Cellular ischemia: ATP depletion
Inflammatory cascade: SIRS in septic shock
🩺 Clinical Features & Investigations
📋 Signs & Symptoms of Shock
✓ Hypotension
SBP <90 mmHg
✓ Tachycardia
HR >100 bpm
✓ Tachypnea
RR >20/min
✓ Cold, clammy skin
(except in distributive shock)
✓ Oliguria
Urine output <0.5 mL/kg/hr
✓ Altered mental status
Confusion, agitation, lethargy
💡 Clinical Pearls
- Early shock: May have normal BP due to compensation
- Pulse pressure: Narrow in hypovolemic, wide in distributive
- Skin signs: Warm in septic/anaphylactic, cold in hypovolemic/cardiogenic
- Capillary refill: >2 seconds indicates poor perfusion
🔬 Investigations in Shock
🩸 Blood tests:
CBC, electrolytes, lactate, ABG
💓 ECG:
Identify MI, arrhythmias
🦠 Cultures:
Blood, urine, sputum if sepsis
📊 Monitoring:
BP, HR, SpO₂, urine output
🩺 Imaging:
CXR, FAST scan, Echo
🧪 Lactate:
>2 mmol/L indicates tissue hypoxia
📈 Key Laboratory Findings
- ABG: Metabolic acidosis (↓ pH, ↓ HCO₃, ↑ lactate)
- CBC: ↑ WBC in sepsis, ↓ Hb in hemorrhage
- Renal function: ↑ Creatinine, BUN in renal hypoperfusion
- Lactate: >4 mmol/L = poor prognosis
🩸 Types of Shock (Detailed)
A. Hypovolemic Shock
⚡ Mechanism
Loss of intravascular volume → ↓ preload → ↓ CO → ↓ tissue perfusion
🎯 Causes
- Hemorrhage (trauma, GI bleed)
- Burns
- Severe dehydration
- Vomiting/diarrhea
💊 Management
- IV fluids (crystalloids)
- Blood transfusion if Hb <7
- Control bleeding source
- Monitor urine output
💡 Key Point: Class I-IV based on blood loss (Class IV: >40% loss). Give 3:1 crystalloid:blood loss ratio.
B. Cardiogenic Shock
⚡ Mechanism
Pump failure → ↓ CO → ↓ tissue perfusion despite adequate volume
🎯 Causes
- Acute MI (most common)
- Heart failure
- Arrhythmias
- Myocarditis
💊 Management
- Oxygen therapy
- Inotropes (dobutamine)
- Revascularization in MI
- Mechanical support (IABP)
💡 Key Point: Mortality >50%. Differentiate from hypovolemic (JVP elevated, pulmonary edema present).
C. Septic Shock
⚡ Mechanism
Infection → SIRS → vasodilation → distributive shock → tissue hypoxia
🎯 Causes
- Gram‑negative bacteria
- Pneumonia, UTI, peritonitis
- Meningitis, cellulitis
- Catheter‑related infections
💊 Management
- Broad‑spectrum antibiotics
- IV fluids (30 mL/kg in first 3h)
- Vasopressors (norepinephrine)
- Source control
💡 Key Point: Defined as sepsis + hypotension despite adequate fluid resuscitation + lactate >2 mmol/L.
📊 Comparison: Hypovolemic vs Cardiogenic vs Septic Shock
| Parameter | Hypovolemic | Cardiogenic | Septic |
|---|---|---|---|
| Skin | Cold, clammy | Cold, clammy | Warm, flushed |
| JVP | Low | High | Variable |
| HR | ↑↑ | ↑ | ↑↑ |
| Primary Rx | Fluids, blood | Inotropes, revascularization | Antibiotics, fluids |
⚡ Other Types of Shock
D. Anaphylactic Shock
Mechanism: IgE‑mediated → histamine release → vasodilation, bronchospasm
Causes: Drugs (penicillin), food (nuts), insect stings, latex
Signs: Urticaria, angioedema, stridor, wheezing
Management:
- Epinephrine 0.3‑0.5 mg IM (first line)
- Antihistamines (H1 & H2 blockers)
- Corticosteroids
- Airway management
E. Neurogenic Shock
Mechanism: Loss of sympathetic tone → vasodilation → ↓ SVR
Causes: Spinal cord injury (T6 or above), spinal anesthesia
Classic triad: Hypotension + Bradycardia + Warm skin
Management:
- IV fluids (cautious)
- Vasopressors (phenylephrine)
- Atropine for bradycardia
- Spinal immobilization
F. Obstructive Shock
Mechanism: Physical obstruction to blood flow → ↓ CO
Causes: PE, cardiac tamponade, tension pneumothorax
Signs: ↑ JVP, muffled heart sounds (tamponade), unilateral absent breath sounds (pneumothorax)
Management:
- Remove obstruction
- Pericardiocentesis (tamponade)
- Chest tube (pneumothorax)
- Anticoagulation/thrombolysis (PE)
G. SIRS (Systemic Inflammatory Response Syndrome)
Definition: Systemic inflammatory response to various insults
Criteria (≥2): Temp >38°C or <36°C, HR >90, RR >20 or PaCO₂ <32 mmHg, WBC >12k or <4k or >10% bands
Progression: SIRS → Sepsis → Severe sepsis → Septic shock → MODS
H. Distributive Shock
Mechanism: Abnormal distribution of blood flow → ↓ SVR
Types: Septic, anaphylactic, neurogenic, adrenal crisis
Hallmark: Warm shock (vasodilation) despite adequate CO
⚡ Electric Shock & Cardiac Effects
Effects on Cardiac Muscle
- Arrhythmias: VT, VF, asystole
- Myocardial damage: Direct thermal injury
- Coronary artery spasm
- Conduction abnormalities
- Cardiac arrest (most common cause of death)
🚨 Mechanism of Cardiac Injury
Electric current → passes through heart → depolarizes myocardium → disrupts electrical conduction → ventricular fibrillation or asystole.
AC vs DC: AC more dangerous (causes tetanic muscle contraction).
Management of Electric Shock
- Scene safety: Turn off power source
- ABC assessment: Airway, Breathing, Circulation
- CPR if pulseless: Start immediately
- ECG monitoring: Minimum 24 hours
- Treat arrhythmias: As per ACLS protocol
- Burn care: Cover entry/exit wounds
- Monitor for rhabdomyolysis: Check CK, urine myoglobin
- Hospital admission: Even if asymptomatic initially
📋 Key Points in Management
- Do NOT touch victim until power off
- Low voltage (<1000V): Usually superficial burns
- High voltage (>1000V): Deep tissue damage, fractures
- Internal injuries: May not be apparent externally
💊 General Management of Shock
Airway
Ensure patent airway
Intubate if GCS ≤8 or respiratory failure
Breathing
High‑flow oxygen (15 L/min)
Target SpO₂ >94%
Ventilatory support if needed
Circulation
IV access (2 large‑bore)
Fluid resuscitation
Control bleeding
Vasopressors if needed
Definitive Care
Treat underlying cause
Antibiotics (sepsis)
Inotropes (cardiogenic)
Epinephrine (anaphylaxis)
📈 Monitoring Parameters in Shock
Vital signs: q15min initially
Urine output: >0.5 mL/kg/hr
Lactate: Clear every 2 hours
CVP: 8‑12 mmHg (if available)
ABG: Monitor pH, HCO₃, PaO₂
Mental status: AVPU scale
Skin perfusion: Capillary refill
Electrolytes: Especially K⁺, Na⁺
📄 ONE PAGE SUMMARY
Types of Shock
- Hypovolemic: Blood/fluid loss → fluids, blood
- Cardiogenic: Pump failure → inotropes
- Septic: Infection → antibiotics, fluids
- Anaphylactic: Allergy → epinephrine
- Neurogenic: Spinal injury → vasopressors
- Obstructive: Physical block → remove obstruction
Key Signs
- Hypotension: SBP <90 mmHg
- Tachycardia: HR >100 bpm
- Oliguria: <0.5 mL/kg/hr
- Altered mentation
- Cold skin: Except in distributive shock
- Lactate: >2 mmol/L
Management (ABCD)
- Airway: Protect, intubate if needed
- Breathing: High‑flow O₂
- Circulation: IV fluids, control bleeding
- Definitive: Treat underlying cause
- Monitor: Vital signs, urine output, lactate
Electric Shock
- Cardiac effects: VF, asystole, MI
- Management: Disconnect power, CPR, ECG monitoring
- Admit: All patients for observation
- Check for: Burns, fractures, rhabdomyolysis
🧠 Memory Aids & Mnemonics
Types of Shock “CHASEN”
Cardiogenic, Hypovolemic, Anaphylactic, Septic, Electric, Neurogenic
Neurogenic Shock Triad
“Brady, Dry, and Warm”
Bradycardia, Dry skin (no sweating), Warm extremities
Septic Shock Bundle “TIME”
Time to antibiotics, IVF resuscitation, Measure lactate, Empiric antibiotics
Anaphylaxis Treatment “EACH”
Epinephrine, Airway, Corticosteroids, H1/H2 blockers
Download Complete Notes
Get a printable PDF with shock classification, management algorithms, and clinical pearls for exams. HA Surgery I Unit 4 Shock Notes
🏷️ Related Topics
Cardiogenic Shock
Septic Shock
Anaphylactic Shock
Neurogenic Shock
Obstructive Shock
SIRS
Electric Shock
Shock Management
Fluid Resuscitation
Vasopressors
Epinephrine
Tissue Perfusion
Lactic Acidosis
MODS
CTEVT Syllabus 2024
Health Science Notes
Surgical Emergencies
Critical Care
Emergency Medicine
Clinical Surgery
© CTEVT Health Science Second Year | Surgery I Unit 4: Shock
Source: CTEVT Syllabus 2024 | For academic use only | Medical emergency requiring immediate intervention. HA Surgery I Unit 4 Shock Notes