HA Surgery I – Unit 3
Emergency Treatment – CTEVT Second Year Notes
According to CTEVT Syllabus (2024) | Health Science (PCL)
Source: aklearningnepal / shekhmdalee
Introduction to Emergency Treatment
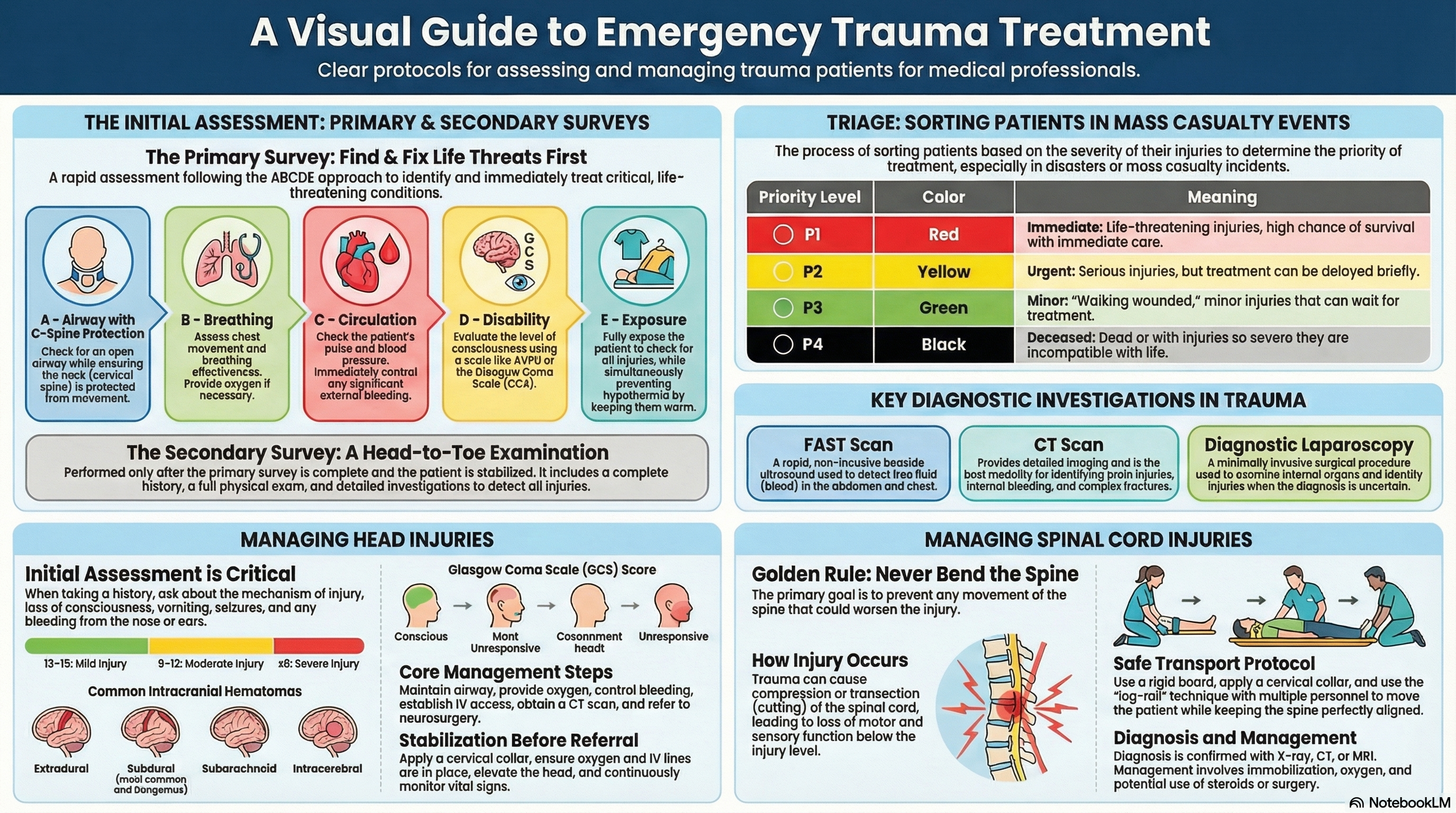
Emergency treatment in surgery focuses on rapid assessment, prioritization, and management of life-threatening conditions. This unit covers systematic approaches to trauma patients, from initial primary survey to definitive care. Mastery of these principles is essential for Health Assistants working in emergency departments, trauma centers, and disaster response situations.
1. Primary and Secondary Survey
Primary Survey (ABCDE Approach)
The immediate assessment to identify and treat life-threatening conditions within the first 2-5 minutes of patient contact.
A – Airway with C-spine
- Assess patency: “Can you speak?”
- Look for obstruction
- Jaw thrust/chin lift (no head tilt if trauma)
- Apply rigid cervical collar
- Suction if needed
B – Breathing
- Look: Chest movement, symmetry
- Listen: Breath sounds
- Feel: Chest expansion
- Rate, effort, oxygen saturation
- Administer O₂ (10-15 L/min via NRB)
C – Circulation
- Check pulse (rate, rhythm)
- BP, capillary refill (>2 sec abnormal)
- Control external bleeding (direct pressure)
- Establish IV access (2 large bore)
- Fluid resuscitation if shocked
D – Disability
- AVPU scale or GCS
- Pupil size and reaction
- Limb movement (purposeful?)
- Blood glucose check
- Signs of raised ICP
E – Exposure/Environment
- Fully undress (cut clothes)
- Log roll for back examination
- Prevent hypothermia (blankets)
- Check for hidden injuries
- Maintain dignity
📌 Key Points:
- Sequence matters: Address each step completely before moving to next
- Reassess frequently: After any intervention, return to A and repeat
- C-spine protection: Assume spinal injury in all trauma until cleared
- Life-threatening conditions: Tension pneumothorax, cardiac tamponade, massive hemorrhage require immediate intervention during primary survey
Secondary Survey
Comprehensive head-to-toe assessment performed after primary survey is complete and patient is stabilized.
Components:
- AMPLE History:
- Allergies
- Medications
- Past medical history
- Last meal
- Events/environment of injury
- Head-to-toe examination: Systematic palpation, inspection, auscultation
- Vital signs: Repeat and monitor trends
- Focused systems review: Based on mechanism of injury
Examination Sequence:
- Head: Scalp, face, eyes, ears, nose, mouth
- Neck: Tracheal position, JVD, crepitus
- Chest: Inspection, palpation, percussion, auscultation
- Abdomen: Tenderness, guarding, distension, bowel sounds
- Pelvis: Stability, tenderness
- Extremities: Deformity, pulses, sensation, movement
- Back: Log roll with spinal precautions
- Neurological: Full GCS, detailed motor/sensory exam
2. Triage in Emergency Cases
Definition: The process of sorting patients based on severity of injury and priority for treatment, especially in mass casualty incidents (MCI) where resources are limited.
Applications: Emergency departments, disaster scenes, battlefield medicine, mass gatherings.
| Color Code | Priority | Patient Condition | Treatment Timeline | Examples |
|---|---|---|---|---|
| RED | Immediate (P1) | Life-threatening but salvageable with immediate intervention | Within minutes | Airway obstruction, tension pneumothorax, severe hemorrhage, GCS ≤8 |
| YELLOW | Urgent (P2) | Serious injuries but stable for short delay | Within 1 hour | Open fractures, major burns without airway compromise, GCS 9-12 |
| GREEN | Delayed/Minor (P3) | Minor injuries, ambulatory (“walking wounded”) | Hours to days | Minor lacerations, sprains, simple fractures, GCS 13-15 |
| BLACK | Expectant/Deceased (P0) | Deceased or unsalvageable with current resources | Comfort care only | Cardiac arrest >20min, severe burns >95%, GCS 3 with fixed pupils |
Triage Principles
- Greatest good for greatest number: In mass casualties, resources go to those most likely to survive
- Dynamic process: Re-triage as patient condition or resource availability changes
- Simple, rapid, reproducible: Use standardized systems (START, SAVE, etc.)
- Clear documentation: Triage tag with color, time, interventions
Triage Methods
- START (Simple Triage and Rapid Treatment): 30-second assessment based on ability to walk, respiratory rate, perfusion, mental status
- JumpSTART: Pediatric version of START
- SALT (Sort, Assess, Lifesaving interventions, Treatment/Transport): Combines sorting and initial interventions
- Emergency Department Triage: Usually 5-level scale (ESI, CTAS, etc.)
3. Investigations in Trauma Victims
FAST Scan
Focused Assessment with Sonography for Trauma
Views: RUQ (Morison’s pouch), LUQ (splenorenal), pericardial, pelvic
Detects: Free fluid (blood) in abdomen, pericardial effusion
CT Scan
Computed Tomography
Indications: Head injury with GCS <15, focal deficit, suspected spine/chest/abdominal injury in stable patient
Protocols: Head, cervical spine, chest/abdomen/pelvis (pan-scan), angiography
Diagnostic Laparoscopy
Minimally Invasive Surgical Exploration
Indications: Equivocal findings, penetrating trauma with possible peritoneal violation, stable patient with suspicion of diaphragm injury
Procedure: General anesthesia, CO₂ insufflation, visual inspection of abdominal cavity
Other Essential Investigations
4. Head Injury
Classification of Head Injuries
By Mechanism
- Closed (blunt): Skull intact, brain injury by acceleration-deceleration
- Open (penetrating): Skull breached (gunshot, stab)
- Crush: Static force compression
- Blast: Pressure wave injury
By Severity (GCS)
- Mild: GCS 13-15, brief LOC (<5 min)
- Moderate: GCS 9-12, LOC 5 min – 6 hours
- Severe: GCS 3-8, LOC >6 hours
By Pathology
- Primary: Immediate mechanical damage (contusion, laceration)
- Secondary: Subsequent processes (edema, ischemia, raised ICP)
History Taking (AMPLE +)
- Mechanism: Height of fall, speed of vehicle, object involved
- Loss of Consciousness: Duration, witnessed?
- Amnesia: Retrograde (before event) vs anterograde (after)
- Vomiting: Frequency, projectile?
- Seizures: Immediate or delayed
- Bleeding: Ear (otorrhea), nose (rhinorrhea), mouth
- Progress: Improving or worsening symptoms
Examination Focus
- Scalp: Lacerations, swelling (boggy = underlying fracture)
- Face: Asymmetry, fractures (raccoon eyes, Battle’s sign = base of skull)
- Eyes: Pupils (size, reaction, anisocoria), eye movements
- Ears/Nose: CSF leak (halo sign on filter paper)
- Neurological: Full GCS, focal deficits, posturing
- Systemic: Signs of raised ICP (Cushing’s triad: HTN, bradycardia, irregular respiration)
Glasgow Coma Scale (GCS)
| Component | Response | Score | Clinical Notes |
|---|---|---|---|
| Eye Opening (E) | Spontaneous | 4 | Eyes open without stimulation |
| To speech | 3 | Open eyes when spoken to | |
| To pain | 2 | Open eyes to painful stimulus | |
| None | 1 | No eye opening despite pain | |
| Verbal Response (V) | Oriented | 5 | Knows who/where/when |
| Confused | 4 | Converses but disoriented | |
| Inappropriate words | 3 | Random or swearing words | |
| Incomprehensible sounds | 2 | Moaning, groaning | |
| None | 1 | No vocalization | |
| Motor Response (M) | Obeys commands | 6 | Follows simple instructions |
| Localizes pain | 5 | Moves hand to remove painful stimulus | |
| Withdrawal from pain | 4 | Pulls away from pain | |
| Flexion to pain (decorticate) | 3 | Abnormal flexion of arms | |
| Extension to pain (decerebrate) | 2 | Arms extended, internally rotated | |
| None | 1 | No movement to pain |
Total GCS = E + V + M (3 to 15). AVPU alternative: Alert, Voice, Pain, Unresponsive.
Intracranial Hematomas
| Type | Location | Mechanism | Classic Presentation | CT Appearance | Management |
|---|---|---|---|---|---|
| Epidural (Extradural) | Between skull and dura | Temporal bone fracture → middle meningeal artery tear | “Lucid interval” (conscious → unconscious), rapid deterioration | Lens-shaped (biconvex), does not cross suture lines | Emergency craniotomy, mortality <10% if treated promptly |
| Acute Subdural | Between dura and arachnoid | Bridging veins rupture (acceleration-deceleration) | Progressive decline, no lucid interval, often associated with brain contusion | Crescent-shaped, crosses suture lines | Craniotomy, mortality ~50-60% due to underlying brain injury |
| Subarachnoid | Subarachnoid space (CSF space) | Traumatic or aneurysmal rupture of cerebral arteries | “Worst headache of life”, neck stiffness, photophobia | High density in basal cisterns, sulci (“white sulci”) | Nimodipine (vasospasm prevention), supportive care, aneurysm clipping if traumatic |
| Intracerebral | Within brain parenchyma | Direct vessel rupture from shearing forces | Focal neurological deficits, raised ICP signs | Irregular high density within brain tissue | Conservative if small, surgery if large/midline shift/ deteriorating |
Skull Fractures
- Linear: Most common, non-displaced, often temporal bone
- Depressed: Bone fragment pushed inward (> skull thickness), may need elevation
- Basilar: Base of skull, signs: raccoon eyes (anterior), Battle’s sign (mastoid), CSF rhinorrhea/otorrhea, cranial nerve deficits
- Compound/open: Overlying scalp laceration, risk of infection
- Growing: In children, fracture widens due to dural tear and CSF pulsation
Immediate Management
- ABCDE with cervical spine protection
- Oxygen to maintain SpO₂ >95%
- IV access, fluids to maintain SBP >90 mmHg
- Control scalp bleeding (direct pressure, staples/sutures)
- Head CT if GCS <15, focal deficit, skull fracture, vomiting, >65 years, coagulopathy
- Neurosurgical consultation for significant findings
Stabilization Before Referral
- Rigid cervical collar (until spine cleared)
- Head elevation 30° (if no spine injury)
- Avoid hyperventilation (unless signs of herniation)
- Mannitol/hypertonic saline if signs of raised ICP
- Seizure prophylaxis (phenytoin/levetiracetam)
- Document serial GCS and pupil checks
5. Spinal Cord Injury
Anatomy Review
Spinal cord segments: Cervical (C1-C8), Thoracic (T1-T12), Lumbar (L1-L5), Sacral (S1-S5), Coccygeal
Spinal cord ends: Conus medullaris at L1-L2 in adults
Cervical enlargement: C5-T1 (brachial plexus, upper limbs)
Lumbar enlargement: L2-S3 (lumbosacral plexus, lower limbs)
Spinal tracts:
- Corticospinal: Motor (anterior = uncrossed, lateral = crossed)
- Spinothalamic: Pain, temperature (crosses immediately)
- Dorsal columns: Vibration, proprioception (crosses in medulla)
- Autonomic: Sympathetic (T1-L2), Parasympathetic (S2-S4)
Pathophysiology
- Primary injury: Mechanical damage at time of trauma (compression, distraction, shear)
- Secondary injury: Ischemia, edema, inflammation, apoptosis (hours to days)
- Spinal shock: Flaccid paralysis, areflexia, hypotension, bradycardia, priapism (lasts days to weeks)
- Neurogenic shock: Loss of sympathetic tone → hypotension with bradycardia (vs hypovolemic shock: tachycardia)
- Autonomic dysreflexia: In injuries above T6, noxious stimulus causes severe HTN, bradycardia, headache (emergency)
Examination (ASIA Scale)
- Motor: Key muscle groups (0-5) bilaterally
- Sensory: Light touch and pinprick in 28 dermatomes
- Reflexes: Initially absent (spinal shock), later hyperreflexia
- Perianal: Sacral sparing (voluntary contraction, sensation) indicates incomplete injury
- Complete vs incomplete: Brown-Séquard, central cord, anterior cord syndromes
Diagnosis
- X-ray: AP, lateral, odontoid views for C-spine
- CT: Gold standard for bony injury
- MRI: Best for cord, ligament, disc injury
- Clearing C-spine: NEXUS criteria or Canadian C-spine Rule
- Indications for imaging: Neck pain, neurological deficit, altered mental status, distracting injury, high-risk mechanism
Management Principles
Transport of Spinal Injury Patient
Golden Rule: “Assume spinal injury until proven otherwise”
- Preparation: Rigid spinal board, cervical collar, head blocks, straps
- Technique: Log roll with at least 3-4 people (one at head maintaining alignment)
- Positioning: Neutral position, no flexion/extension/rotation
- Monitoring: Neurological status before, during, after movement
Special Considerations
- Helmet removal: Only if airway compromised, preferably by two trained persons
- Extrication: From vehicle: maintain alignment, use Kendrick extrication device if available
- Long transports: Pressure care (padded board), frequent neuro checks
- Children: Larger head → use padding under torso to maintain neutral position
One Page Summary: Emergency Treatment
• A: Airway + C-spine
• B: Breathing + O₂
• C: Circulation + bleeding control
• D: Disability (GCS/AVPU)
• E: Exposure + prevent hypothermia
• Treat life threats immediatelySECONDARY SURVEY
• After primary, head-to-toe exam
• AMPLE history
• Detailed systems examination
• Appropriate investigations
TRIAGE (Colors)
• Red: Immediate (minutes)
• Yellow: Urgent (1 hour)
• Green: Delayed (hours)
• Black: Expectant/deceased
• START method for mass casualties
TRAUMA INVESTIGATIONS
• FAST: Free fluid in abdomen
• CT: Gold standard for most
• X-ray: C-spine, chest, pelvis
• Diagnostic laparoscopy: equivocal cases
HEAD INJURY – GCS
• Eye (1-4), Verbal (1-5), Motor (1-6)
• Mild: 13-15, Moderate: 9-12, Severe: 3-8
• AVPU: Alert, Voice, Pain, Unresponsive
• Epidural: Lens-shaped, lucid interval
• Subdural: Crescent-shaped, worse prognosis
• Subarachnoid: “Worst headache”, blood in CSF spaces
• Intracerebral: Within brain tissueSKULL FRACTURES
• Linear: Most common
• Depressed: May need elevation
• Basilar: Raccoon eyes, Battle’s sign, CSF leak
HEAD INJURY MANAGEMENT
• ABCDE, C-spine protection
• Oxygen, IV access, control bleeding
• CT head if indicated
• Neurosurgical referral
• Elevate head 30°, mannitol if raised ICP
SPINAL CORD INJURY
• Immobilize (collar, board, log roll)
• Assume injury until cleared
• Spinal shock: flaccid, areflexic, hypotensive
• Neurogenic shock: hypotension + bradycardia
• MRI best for cord injury
• Methylprednisolone within 8h (controversial)
TRANSPORT
• Never bend/twist spine
• Log roll with 3-4 people
• Maintain neutral alignment
• Monitor neurological status
Life before limb, ABCDE first, C-spine protection in all trauma
Visual Aid: ABCDE Approach Algorithm
Topic Tags
ABCDE Approach
Triage
Mass Casualty
FAST Scan
Head Injury
Glasgow Coma Scale
Epidural Hematoma
Subdural Hematoma
Skull Fracture
Spinal Cord Injury
Spinal Immobilization
Log Roll Technique
Trauma Management
Emergency Treatment
CTEVT Syllabus
Health Assistant
Trauma Nursing
Secondary Survey
HA Second Year
Key Clinical Takeaways
- Primary survey follows strict ABCDE sequence; treat life threats immediately as they are identified.
- Triage prioritizes patients based on severity and survivability, especially in mass casualty incidents.
- FAST scan is a rapid bedside tool for detecting intra-abdominal free fluid in trauma.
- GCS is the standard for assessing consciousness; document each component separately.
- Epidural hematoma classically presents with lucid interval; subdural has worse prognosis due to underlying brain injury.
- Assume spinal injury in all trauma patients until properly cleared; immobilize with collar and log roll technique.
Quick Self-Check
Question 1: In the ABCDE approach, what does “C” stand for and what are the key actions?
Question 2: Match the triage color to its priority:
1. Red
2. Yellow
3. Green
Further Reading & Resources
- Official CTEVT Syllabus: CTEVT Website
- ATLS (Advanced Trauma Life Support) Manual: ATLS Guidelines
- Brain Trauma Foundation Guidelines: Brain Trauma Guidelines