HA Surgery I – Unit 2
Wound and Hemorrhage – CTEVT Second Year Notes
According to CTEVT Syllabus (2024) | Health Science (PCL)
Source: aklearningnepal / shekhmdalee
Introduction
Wound and hemorrhage management are fundamental surgical skills for Health Assistants. This unit covers the classification, pathophysiology, and clinical management of various wounds and bleeding conditions. Understanding these principles is essential for preventing complications, promoting healing, and saving lives in emergency situations.
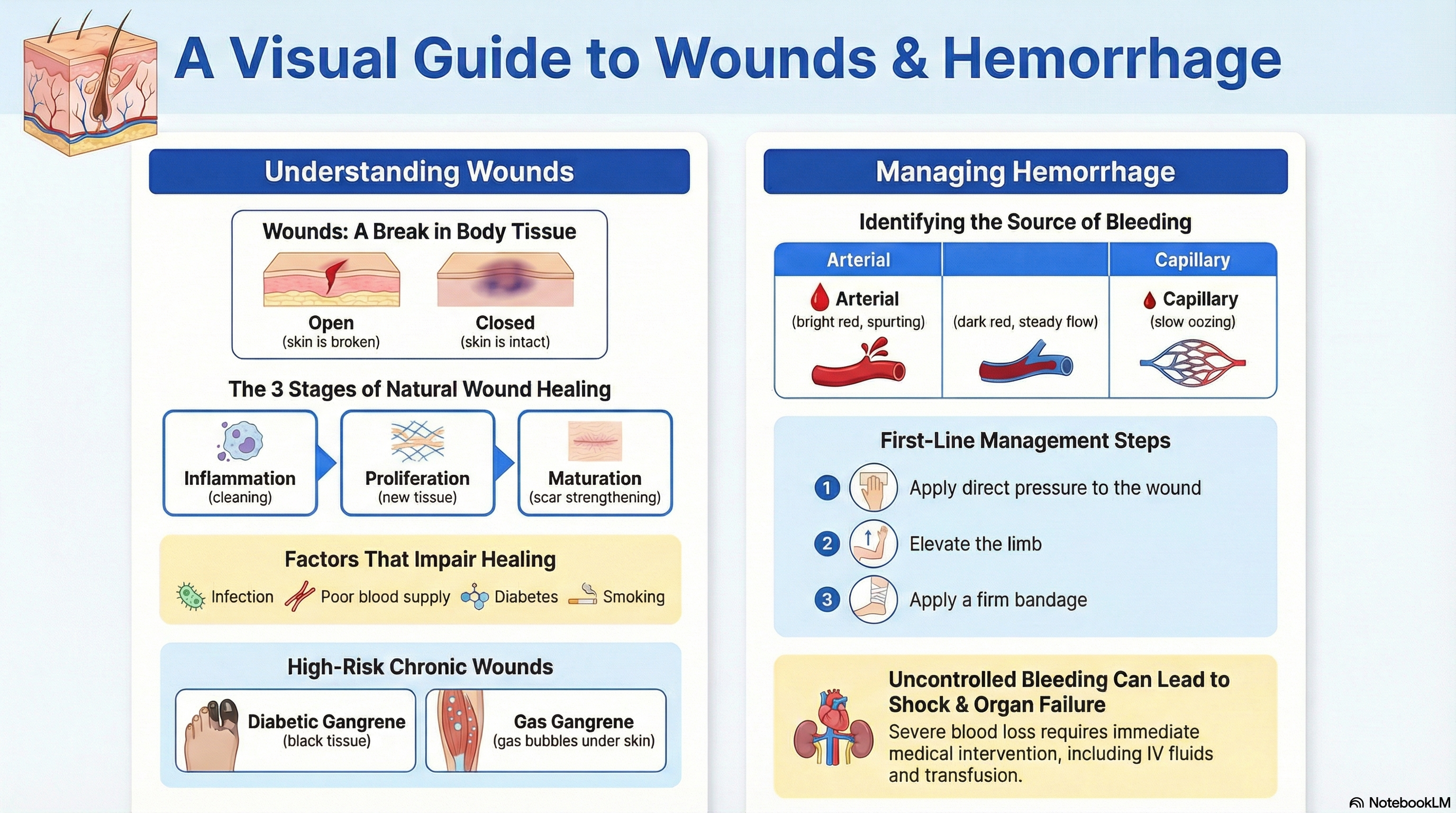
1. WOUNDS: Classification & Management
Definition
A wound is a break or disruption in the continuity of skin or body tissues caused by injury, trauma, surgery, or disease.
Open Wounds
- Incised: Clean cut by sharp object (scalpel, glass) – edges regular
- Lacerated: Irregular tear by blunt force – edges jagged
- Abrasion: Superficial scrape – epidermis damaged
- Puncture: Deep, narrow wound (nail, needle) – high infection risk
- Avulsion: Tissue forcibly torn away
- Penetrating: Entering body cavity (gunshot, stab)
Closed Wounds
- Contusion (Bruise): Blunt trauma → capillary rupture, blood extravasation
- Hematoma: Localized collection of blood outside vessels
- Crush Injury: Compression force → tissue damage
- Internal Injury: Damage to internal organs without skin breach
Clinical Features of Wounds
| Sign/Symptom | Clinical Significance |
|---|---|
| Pain | Varies with wound type and location; nerve damage may reduce pain |
| Bleeding | Depends on vessel type; arterial = bright red, spurting; venous = dark, steady |
| Swelling (Edema) | Inflammatory response; increases in first 48-72 hours |
| Redness (Erythema) | Local inflammation; spreading redness suggests infection |
| Loss of Function | Due to pain, tissue damage, or nerve/tendon injury |
| Signs of Infection | Pus, fever >38°C, foul odor, increasing pain, lymphangitis |
Management of Different Wounds
Clean Minor Wound
- Wash with normal saline
- Apply antiseptic (povidone-iodine)
- Simple dressing
- Tetanus prophylaxis if needed
Deep/Bleeding Wound
- Direct pressure to stop bleeding
- Wound exploration & irrigation
- Layered suturing if needed
- Antibiotics (if contaminated)
- Tetanus prophylaxis
Dirty/Infected Wound
- Thorough debridement
- Leave open/delayed closure
- Broad-spectrum antibiotics
- Regular dressing changes
- Wound culture if needed
Tetanus-Prone Wound
- Wounds >6 hours old
- Contaminated with soil/feces
- Puncture/avulsion wounds
- Give tetanus toxoid ± immunoglobulin
Normal Wound Healing Stages
Immediate – 6 hours
Vasoconstriction → Platelet plug → Clot formation
6 hrs – 5 days
Redness, swelling, heat, pain
Neutrophils → Macrophages
3-21 days
Granulation tissue
Angiogenesis & collagen deposition
3 weeks – 2 years
Collagen remodeling
Scar strength increases
Mnemonic: He Inflamed Purple Mat (Hemostasis, Inflammation, Proliferation, Maturation)
Factors Affecting Wound Healing
Local Factors
- Infection: Most common cause of delayed healing
- Poor Blood Supply: Arterial/venous insufficiency
- Foreign Bodies: Retained fragments, sutures
- Movement/Tension: Disrupts healing edges
- Radiation Damage: Fibrotic, hypoxic tissue
- Moisture Balance: Too dry or too wet
Systemic Factors
- Age: Slower healing in elderly
- Malnutrition: Protein, vitamin C, zinc deficiency
- Diabetes: Microvascular disease, immune dysfunction
- Anemia: Reduced oxygen delivery
- Smoking: Vasoconstriction, ↓ oxygen
- Immunosuppression: Steroids, chemotherapy, HIV
2. CHRONIC WOUNDS
Chronic wounds are those that fail to progress through normal healing stages within 4-6 weeks due to underlying pathology.
| Type | Etiology/Causes | Clinical Features | Management | Complications |
|---|---|---|---|---|
| Pressure Sores (Bed Sores/Decubitus) |
• Continuous pressure (bony prominences) • Shear/friction forces • Immobility (paralysis, coma) • Moisture (incontinence) • Poor nutrition |
Stages: I: Non-blanchable erythema II: Partial thickness loss III: Full thickness loss IV: Exposed bone/tendon Pain, infection signs |
• Pressure relief (2-hour turns) • Special mattresses • Debridement of necrotic tissue • Moist wound dressings • Nutritional support • Antibiotics if infected |
• Cellulitis • Osteomyelitis • Sepsis • Marjolin’s ulcer (SCC) • Death |
| Leg Ulcers | Venous (70%): Venous HTN, DVT, varicose veins Arterial (10%): PAD, atherosclerosis, diabetes Mixed (10-15%): Both venous & arterial Other: Vasculitis, infection, malignancy |
Venous: Medial malleolus, shallow, painless, edema, hemosiderin staining Arterial: Distal toes/feet, deep, painful, pale base, no edema Exudate, odor, surrounding skin changes |
• Compression therapy (venous) • Limb elevation • Debridement • Moist dressings • Antibiotics if infected • Vascular surgery if arterial |
• Chronic infection • Cellulitis • Osteomyelitis • Malignant transformation • Amputation (arterial) |
| Diabetic Foot Ulcer/Gangrene |
• Peripheral neuropathy (loss of sensation) • Peripheral arterial disease • Immunopathy (impaired healing) • Infection (often polymicrobial) • Trauma (unnoticed due to neuropathy) |
• Neuropathic: Painless, plantar surface, callus • Ischemic: Painful, distal, pale • Wet gangrene: Swollen, discolored, foul odor • Dry gangrene: Black, mummified, well-demarcated • Probe to bone test positive for osteomyelitis |
• Glycemic control • Off-loading (special footwear) • Debridement • Antibiotics (broad spectrum) • Vascular assessment • Amputation if non-salvageable |
• Osteomyelitis • Sepsis • Systemic infection • Amputation • Death (5-year mortality ~50%) |
| Gas Gangrene | • Clostridium perfringens (anaerobic) • Contaminated traumatic wounds • Post-surgical (bowel/biliary surgery) • Ischemic tissue (arterial insufficiency) • Immunocompromised states |
• Sudden onset severe pain • Swelling, pale then bronze/dark skin • Crepitus (gas bubbles in tissue) • Foul-smelling serosanguinous discharge • Systemic toxicity: fever, tachycardia, hypotension • Rapid progression (hours) |
Surgical Emergency: • Immediate radical debridement/amputation • High-dose IV penicillin + clindamycin • Hyperbaric oxygen if available • ICU support for sepsis • Tetanus prophylaxis |
• Septic shock • Multi-organ failure • Disseminated intravascular coagulation • High mortality (25-40%) • Limb loss even with treatment |
📌 Clinical Tips for Chronic Wounds
3. SCARS: Types and Management
Definition
A scar is the fibrous tissue that replaces normal tissue after injury or surgery. It’s composed primarily of collagen type III (later replaced by type I).
Normal Fine-Line Scar
Matures over 6-18 months to pale, flat, supple line.
Hypertrophic Scar
Raised, red, itchy but confined to wound boundaries. Common in wounds under tension.
Keloid Scar
Grows beyond wound margins, persistent, familial tendency, common in darker skin.
Atrophic Scar
Sunken/depressed (acne, chickenpox, steroid use). Loss of collagen.
Contracture Scar
Shortening causing functional limitation (burns, across joints).
Stretched Scar
Widened, flat, often on abdomen, back, or after pregnancy.
Scar Management Principles
4. HEMORRHAGE: Classification & Management
Definition
Hemorrhage is the escape of blood from the cardiovascular system, which can be external or internal, arterial, venous, or capillary.
Classification of Hemorrhage
By Vessel Type
- Arterial: Bright red, spurts synchronously with pulse, difficult to control
- Venous: Dark red, steady flow, easier to control
- Capillary: Bright red, oozing, multiple pinpoint sources
- Parenchymal: From solid organs (liver, spleen), oozing from cut surface
By Timing
- Primary: At time of injury
- Reactionary: Within 24h (BP rise, dislodged clot, vasodilatation after warming)
- Secondary: 7-14 days later (infection, sloughing of clot, vessel erosion)
By Visibility
- External/Revealed: Obvious bleeding (hematemesis, epistaxis, wound)
- Internal/Concealed: Hidden (intracranial, intra-abdominal, intramuscular)
- Bruise/Ecchymosis: Bleeding into skin/subcutaneous tissue
Management of Hemorrhage – Stepwise Approach
Direct Pressure
Use sterile gauze/pad
Elevation
Above heart level
Pressure Points
Brachial/femoral artery
Tourniquet
Last resort for limb injury
IV Access
Large bore cannula
Fluid Resuscitation
Crystalloids → blood
Surgical Control
Ligation, packing, repair
Remember: ABCDE approach (Airway, Breathing, Circulation, Disability, Exposure) always first.
Effects and Complications of Hemorrhage
Acute Effects (Hemorrhagic Shock)
- Class I (<15%): Mild tachycardia, normal BP
- Class II (15-30%): Tachycardia, tachypnea, anxiety
- Class III (30-40%): Hypotension, confusion, oliguria
- Class IV (>40%): Profound shock, unconscious, anuria
Systemic Complications
- Hypovolemic Shock: Inadequate tissue perfusion
- Acute Kidney Injury: Renal hypoperfusion
- Myocardial Ischemia: Reduced coronary flow
- Cerebral Hypoxia: Confusion → coma
- Coagulopathy: Dilutional, consumption (DIC)
Chronic/Late Effects
- Anemia: Reduced oxygen-carrying capacity
- Fatigue, Dyspnea: Compensatory mechanisms
- Infection Risk: Immunosuppression from stress
- Organ Dysfunction: If prolonged shock occurred
- Psychological: PTSD, anxiety disorders
One Page Summary: Key Points
• Open: Incised, lacerated, abrasion, puncture
• Closed: Contusion, hematomaWOUND HEALING STAGES
• Hemostasis (immediate)
• Inflammation (6h-5d)
• Proliferation (3-21d)
• Maturation (3w-2y)
Mnemonic: He Inflamed Purple MatFACTORS AFFECTING HEALING
• Local: Infection, poor blood supply, FB
• Systemic: Age, diabetes, malnutrition, smoking
CHRONIC WOUNDS
• Pressure sores: Immobility, staging I-IV
• Leg ulcers: Venous (medial), arterial (distal)
• Diabetic foot: Neuropathic/ischemic
• Gas gangrene: Clostridium, surgical emergency
SCAR TYPES
• Normal, hypertrophic, keloid, atrophic
• Contracture: Functional limitation
• Stretched: Widened, on abdomen
• Silicone sheets/gel (early)
• Steroid injections (hypertrophic/keloid)
• Surgery + radiation (keloid)
• Physiotherapy (contracture)HEMORRHAGE TYPES
• Arterial: Bright red, spurting
• Venous: Dark red, steady
• Capillary: Oozing
• Primary: At injury
• Reactionary: Within 24h
• Secondary: After 7-14dHEMORRHAGE MANAGEMENT
• Direct pressure → elevation → pressure points
• Tourniquet (last resort)
• IV fluids (crystalloids first)
• Blood transfusion if significant loss
• Surgical control (ligation, packing)
CLINICAL MNEMONICS
• SIRS criteria: Temp >38 or <36, HR >90, RR >20, WBC >12 or <4
• Shock classes: I (<15%), II (15-30%), III (30-40%), IV (>40%)
• Tetanus-prone: >6h old, contaminated, puncture, avulsion
ABC first → Control bleeding → Prevent infection → Promote healing
Topic Tags
Hemorrhage Control
Chronic Wounds
Pressure Sores
Leg Ulcers
Diabetic Foot
Gas Gangrene
Scar Management
Keloid
Wound Healing
Hemorrhage Types
Shock Management
Debridement
Tetanus Prophylaxis
CTEVT Syllabus
Health Assistant
Surgical Nursing
Wound Infection
Trauma Care
HA Second Year
Key Clinical Takeaways
- Wound assessment includes type, depth, contamination, vascular/neurological status, and infection signs.
- Chronic wounds require treatment of underlying cause (pressure relief, compression, glycemic control).
- Gas gangrene is a surgical emergency requiring immediate debridement and antibiotics.
- Scar management begins with prevention through proper wound closure and continues with silicone, steroids, or surgery.
- Hemorrhage control follows stepwise approach: direct pressure → elevation → pressure points → tourniquet (last).
- Always assess for tetanus risk and provide prophylaxis for contaminated or old wounds.
Quick Self-Check
Question 1: Which type of hemorrhage is characterized by bright red, spurting blood?
Question 2: Match the wound type to its description:
1. Incised wound
2. Pressure sore
3. Keloid scar
Further Reading & Resources
- Official CTEVT Syllabus: CTEVT Website
- WHO Guidelines on Wound Care: WHO Wound Management
- Advanced Trauma Life Support (ATLS) Manual: ATLS Guidelines