HA Pharmacology And Pharmacy – Unit 5
Drugs Used in Cardiovascular System – CTEVT Second Year Notes
According to CTEVT Syllabus (2024) | Health Science (PCL)
Introduction to Cardiovascular Drugs
Cardiovascular drugs are among the most commonly prescribed medications worldwide, used to treat conditions like hypertension, heart failure, angina, dyslipidemia, and thromboembolic disorders. Understanding their mechanisms, indications, and adverse effects is crucial for Health Assistants involved in patient care, medication administration, and patient education.
1. ANTIHYPERTENSIVE DRUGS
A. DIURETICS
B. ACE INHIBITORS
| Drug | Mechanism | Indications | Key Side Effects | Dose |
|---|---|---|---|---|
| Captopril | Inhibits ACE → ↓ Angiotensin II → vasodilation | HTN, CHF, post-MI, diabetic nephropathy | Dry cough, hyperkalemia, angioedema, rash | 25–50 mg BD (start 12.5 mg) |
| Enalapril | Prodrug → enalaprilat; long-acting ACE inhibition | HTN, CHF, asymptomatic LV dysfunction | Cough, hyperkalemia, dizziness, fatigue | 5–40 mg daily |
| Ramipril | Long-acting; tissue protective effects | HTN, CHF post-MI, CV risk reduction | Cough, dizziness, hyperkalemia, hypotension | 2.5–10 mg daily |
C. ANGIOTENSIN II RECEPTOR BLOCKERS (ARBs)
Losartan
Mechanism: Selective AT1 receptor antagonist
Indications: HTN, diabetic nephropathy, stroke prevention
Side Effects: Dizziness, hyperkalemia, rarely angioedema
Dose: 50–100 mg daily
Telmisartan
Mechanism: Long-acting AT1 blocker with PPAR-γ activity
Indications: HTN, CV risk reduction, metabolic syndrome
Side Effects: Back pain, diarrhea, hyperkalemia
Dose: 40–80 mg daily
D. CALCIUM CHANNEL BLOCKERS
| Drug | Class | Mechanism | Key Indications | Side Effects | Dose |
|---|---|---|---|---|---|
| Nifedipine | Dihydropyridine | Blocks L-type Ca²⁺ channels → arterial vasodilation | HTN, chronic stable angina, vasospastic angina | Headache, flushing, edema, reflex tachycardia | 30–90 mg SR daily |
| Amlodipine | Dihydropyridine | Long-acting arterial vasodilation | HTN, chronic stable angina | Peripheral edema, headache, dizziness | 5–10 mg once daily |
E. BETA-ADRENERGIC BLOCKERS
Propranolol
Type: Non-selective (β₁ + β₂)
Indications: HTN, angina, arrhythmias, migraine, anxiety
Side Effects: Bradycardia, bronchospasm, fatigue, depression
Contraindications: Asthma, heart block, cardiogenic shock
Dose: 40–160 mg daily
Metoprolol
Type: Selective β₁ (cardioselective)
Indications: HTN, angina, CHF, post-MI, arrhythmias
Side Effects: Fatigue, bradycardia, dizziness, insomnia
Contraindications: Cardiogenic shock, severe bradycardia
Dose: 50–200 mg daily
Atenolol
Type: Selective β₁ (hydrophilic)
Indications: HTN, angina, arrhythmias
Side Effects: Bradycardia, fatigue, cold extremities
Contraindications: Severe bradycardia, heart block
Dose: 25–100 mg once daily
2. ANTI-ANGINAL DRUGS
Nitroglycerin (Glyceryl Trinitrate)
Mechanism: Converts to NO → activates guanylyl cyclase → ↑ cGMP → vasodilation (venous > arterial)
Indications: Acute angina attacks, prophylaxis, hypertensive emergencies
Side Effects: Headache, hypotension, reflex tachycardia, tolerance
Contraindications: Severe anemia, hypotension, phosphodiesterase inhibitor use
Dose: SL: 0.3–0.6 mg; IV: 5–200 mcg/min
3. CARDIAC GLYCOSIDES
Digoxin
Mechanism: Inhibits Na⁺/K⁺ ATPase → ↑ intracellular Ca²⁺ → positive inotropy; ↑ vagal tone
Indications: Heart failure with reduced EF, atrial fibrillation rate control
Process of Digitalization:
- Loading: 0.5–1 mg over 24h in divided doses
- Maintenance: 0.125–0.25 mg daily
Toxicity Symptoms: Nausea, vomiting, confusion, yellow halos (xanthopsia), arrhythmias
Treatment of Toxicity: Stop digoxin, correct K⁺, Digibind (digoxin-specific antibodies)
Contraindications: Ventricular tachycardia, heart block (unless paced), WPW
Dose: Maintenance 0.125–0.25 mg daily
4. LIPID-LOWERING DRUGS
Atorvastatin (Statins)
Mechanism: Inhibits HMG-CoA reductase → ↓ cholesterol synthesis → ↑ LDL receptors
Indications: Hypercholesterolemia, CVD prevention, post-MI, stroke prevention
Side Effects: Myalgia, elevated LFTs, rare rhabdomyolysis, increased glucose
Contraindications: Active liver disease, pregnancy, lactation
Dose: 10–80 mg once daily
Fenofibrate (Fibrates)
Mechanism: Activates PPAR-α → ↑ lipoprotein lipase → ↓ triglycerides, ↑ HDL
Indications: Hypertriglyceridemia, mixed dyslipidemia
Side Effects: GI upset, myopathy, gallstones, elevated creatinine
Contraindications: Severe renal/hepatic disease, gallbladder disease
Dose: 160 mg daily or 54–145 mg based on formulation
5. OTHER CARDIOVASCULAR DRUGS
| Drug | Mechanism/Class | Indications | Key Side Effects | Dose |
|---|---|---|---|---|
| Labetalol | α₁ + non-selective β blocker | Hypertensive emergencies, pregnancy-induced HTN | Orthostatic hypotension, bronchospasm, fatigue | Oral: 100–400 mg BD; IV: 20–80 mg bolus |
| Prazosin | Selective α₁ blocker | HTN, BPH, Raynaud’s, PTSD nightmares | First-dose syncope, dizziness, palpitations | 1–20 mg daily divided |
| Phentolamine | Non-selective α blocker | Pheochromocytoma diagnosis/treatment, extravasation | Hypotension, tachycardia, arrhythmias | 5 mg IV for pheochromocytoma |
| Methyldopa | Centrally acting α₂ agonist | HTN in pregnancy, essential HTN | Sedation, dry mouth, hepatitis, +Coombs test | 250 mg–2 g daily divided |
| Mannitol | Osmotic diuretic | Cerebral edema, increased IOP, oliguric renal failure | Fluid overload, hyponatremia, headache, nausea | 0.5–2 g/kg IV over 30–60 min |
| Vasopressin (ADH) | V1/V2 receptor agonist | Diabetes insipidus, GI bleeding, vasodilatory shock | Hypertension, water intoxication, angina | 5–40 units IM/SC/IV; shock: 0.01–0.1 units/min |
| Aspirin | Irreversible COX-1 inhibitor | MI/stroke prevention, pain, inflammation, fever | GI bleeding, tinnitus, Reye’s syndrome, allergy | 75–325 mg daily (CV prevention) |
| Clopidogrel | Irreversible P2Y12 inhibitor | Post-stent, ACS, stroke prevention (if aspirin allergic) | Bleeding, rash, diarrhea, TTP | 75 mg daily; load: 300–600 mg |
| Heparin | Activates antithrombin III | DVT/PE treatment/prophylaxis, ACS, catheter patency | Bleeding, HIT, osteoporosis (long-term) | Prophylaxis: 5000 units SC q8–12h |
| Warfarin | Vitamin K epoxide reductase inhibitor | DVT/PE, atrial fibrillation, mechanical heart valves | Bleeding, skin necrosis, teratogenicity | 2–10 mg daily (adjust to INR 2–3) |
| Vitamin K | Cofactor for clotting factors synthesis | Warfarin overdose, vitamin K deficiency | Allergy, anaphylaxis (IV), hyperbilirubinemia (newborns) | 1–10 mg oral/IV/IM; warfarin reversal: 2.5–10 mg |
📌 Clinical Tips & Important Notes
Memory Aids & Mnemonics
C = Cough, A = Angioedema, P = Potassium ↑, T = Taste disturbance, O = Orthostatic hypotension, P = Proteinuria, R = Rash, I = Impotence, L = Low BP
D = Diplopia, I = Intestinal (N/V/D), G = Green/yellow vision, O = Others (confusion, fatigue), X = X-tra cardiac (arrhythmias), I = Impotence, N = Nausea
A = Asthma/COPD, B = Bradycardia/Block, C = Cardiogenic shock, D = Decompensated heart failure
V = Vitamin K (oral/IV), I = INR check, P = Prothrombin complex concentrate/FFP for major bleeding
One Page Summary: Key Points
• HCTZ: Distal tubule, hypokalemia, hyperglycemia
• Furosemide: Loop diuretic, ototoxicity, hypokalemia
• Spironolactone: K⁺-sparing, hyperkalemia, gynecomastia
• Acetazolamide: Carbonic anhydrase inhibitor, metabolic acidosisACE INHIBITORS
• Captopril, Enalapril, Ramipril
• Dry cough, angioedema, hyperkalemia
• Contraindicated in pregnancy, bilateral renal artery stenosis
ARBs
• Losartan, Telmisartan
• No cough, similar indications to ACEI
• Same contraindications as ACEI
CALCIUM CHANNEL BLOCKERS
• Nifedipine: Dihydropyridine, edema, headache
• Amlodipine: Long-acting, edema common
• Verapamil/Diltiazem: Non-DHP, constipate, bradycardia
BETA BLOCKERS
• Propranolol: Non-selective, asthma caution
• Metoprolol: β₁ selective, CHF, post-MI
• Atenolol: Hydrophilic, once daily
• Avoid in asthma, heart block, decompensated CHF
• Nitroglycerin: NO donor, SL for acute attack, headache
• Tolerance with continuous useCARDIAC GLYCOSIDES
• Digoxin: Na⁺/K⁺ ATPase inhibitor, positive inotropy
• Toxicity: N/V, confusion, yellow vision, arrhythmias
• Digitalization: Load then maintain
LIPID-LOWERING
• Statins (atorvastatin): HMG-CoA reductase inhibition, myalgia
• Fibrates (fenofibrate): ↓ triglycerides, ↑ HDL, gallstones
OTHER CV DRUGS
• Labetalol: α+β blocker, pregnancy HTN
• Prazosin: α₁ blocker, first-dose syncope
• Aspirin: Antiplatelet, GI bleed risk
• Clopidogrel: P2Y12 inhibitor, post-stent
• Heparin: AT III activation, HIT risk
• Warfarin: Vitamin K antagonist, INR monitoring
• Vitamin K: Warfarin reversal
MONITORING
• Electrolytes with diuretics
• Renal function with ACEI/ARB
• Digoxin levels
• LFTs with statins
• INR with warfarin
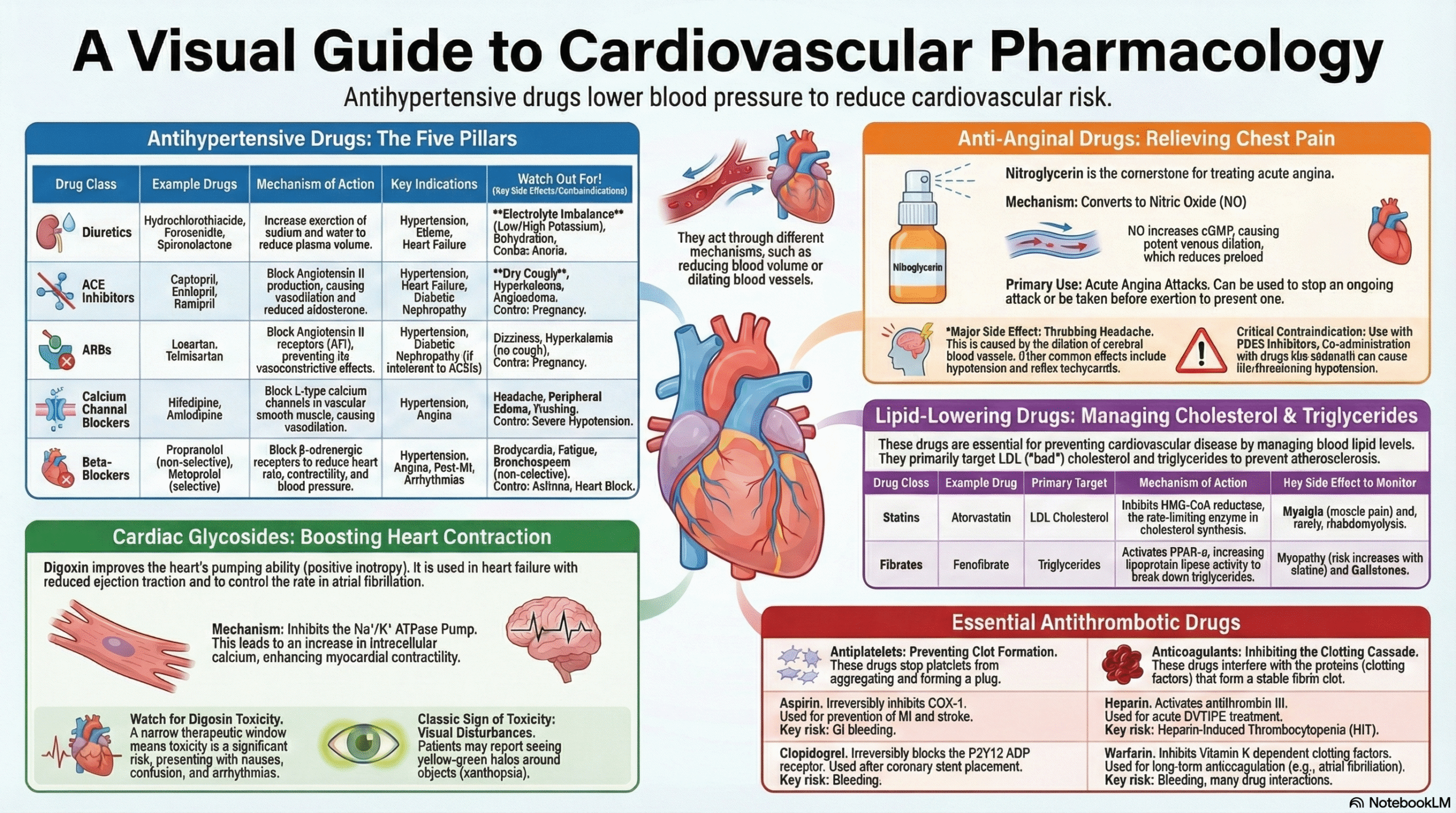
Start low, go slow with antihypertensives. Monitor for orthostasis, electrolyte imbalances, and renal function.
Visual Aid: Antihypertensive Drug Classes Mechanism
Topic Tags
Diuretics
ACE Inhibitors
ARBs
Beta Blockers
Calcium Channel Blockers
Nitroglycerin
Digoxin
Statins
Antiplatelet Drugs
Anticoagulants
Heart Failure Drugs
Hypertension Management
Lipid Lowering Drugs
Cardiovascular Pharmacology
CTEVT Syllabus
Health Assistant
HA Second Year
Pharmacology Notes
Medical Education
Key Clinical Takeaways
- Hypertension management often requires combination therapy; thiazide diuretics are excellent for combination.
- ACE inhibitor cough occurs in significant proportion; switch to ARB if intolerable.
- Digoxin has narrow therapeutic window; monitor for toxicity especially in elderly and renal impairment.
- Statins are first-line for LDL lowering; monitor LFTs and CK for muscle symptoms.
- Warfarin requires regular INR monitoring and has numerous food/drug interactions.
- Antiplatelet therapy (aspirin/clopidogrel) is crucial in CAD, post-stent, and stroke prevention.
Quick Self-Check
Question 1: Which diuretic is most likely to cause hyperkalemia?
Question 2: Match the drug to its characteristic side effect:
1. ACE inhibitors
2. Digoxin
3. Nitroglycerin
Download Notes
Get a printable PDF version of these comprehensive cardiovascular pharmacology notes. HA Pharmacology and Pharmacy Unit 5 Drugs Used in Cardiovascular System Notes
Includes all drug classes, mechanisms, doses, and clinical tips. HA Pharmacology and Pharmacy Unit 5 Drugs Used in Cardiovascular System Notes
Further Reading & Resources
- Official CTEVT Syllabus: CTEVT Website
- American Heart Association Guidelines: AHA Guidelines
- European Society of Cardiology: ESC Guidelines