Basic Medical Procedure and First Aid
General Medicine (HA) – Second Year
Unit 1: History Taking and Physical Examination
A Systematic Approach to Patient Assessment
Why This Unit Matters
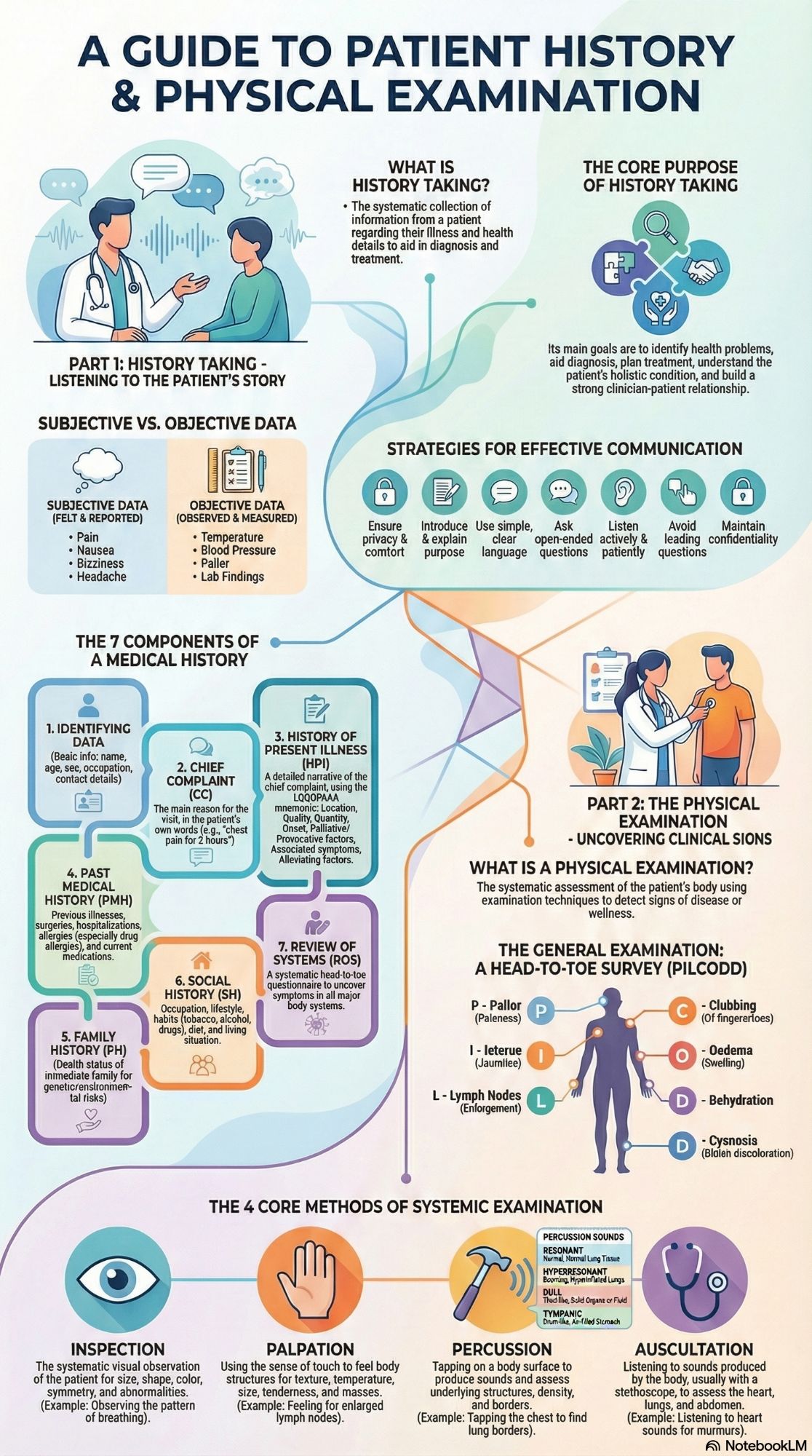
History taking and physical examination form the cornerstone of clinical medicine. Over 70% of diagnoses can be made from a thorough history alone, with physical examination contributing significantly to the remaining percentage. This unit teaches the systematic approach that ensures comprehensive patient assessment while building therapeutic relationships.
Mastering these skills is essential for all healthcare professionals, particularly in resource-limited settings where advanced diagnostic tools may not be readily available. The techniques described here follow internationally recognized standards adapted from sources like CTEVT Nepal and standard medical textbooks.
A. History Taking
1. Definition & Purpose
History taking is the systematic collection of information from a patient or attendant regarding present illness, past illness, and other relevant health details to aid in diagnosis and treatment.
Main purposes:
- Identify the patient’s health problems
- Help in accurate diagnosis
- Plan appropriate investigations and treatment
- Understand the patient’s physical, psychological, and social condition
- Establish good nurse-patient / health worker-patient relationship
3. Subjective vs. Objective Data
| Subjective Data | Objective Data |
|---|---|
| Information felt and reported by the patient | Information that can be observed, measured, or verified |
| Cannot be directly measured | Collected by physical examination or investigations |
Examples:
|
Examples:
|
📝 Memory Aid: LQQOPAAA for History of Present Illness
Use this mnemonic to ensure comprehensive history of present illness:
Location • Quality • Quantity/Severity • Onset • Precipitating/Palliating • Aggravating • Alleviating • Associated symptoms
5. Components of History Taking (The Medical History)
- Identifying Data: Name, age, sex, occupation, contact
- Chief Complaint (CC): Main reason in patient’s words
- History of Present Illness (HPI): Detailed chronological narrative using LQQOPAAA
- Past Medical History (PMH): Illnesses, surgeries, allergies, medications
- Family History (FH): Health of immediate family
- Social History (SH): Occupation, lifestyle, habits, living situation
- Review of Systems (ROS): Systematic questioning of all body systems
B. Physical Examination
1. Definition & Purpose
Physical examination is the systematic assessment of the patient’s body using observation and examination techniques to detect signs of disease.
Purposes include: identifying physical signs, confirming diagnostic hypotheses, detecting asymptomatic conditions, assessing severity, monitoring changes, and establishing baselines.
3. General Examination: Head-to-Toe Approach (PILCODD)
A systematic mnemonic for general survey:
Pallor: Check conjunctiva, tongue, nailsI
Icterus: Yellow sclera, skin, under tongue
L
Lymph Nodes: Palpate cervical, axillary, inguinal
C
Clubbing: Loss of nail bed angle
O
Oedema: Dependent swelling, check for pitting
D
Dehydration: Skin turgor, dry mouth, sunken eyes
D
Cyanosis: Bluish lips, tongue, extremities
5. Methods of Systemic Examination
A. Inspection
Systematic visual observation
Observe: size, shape, color, symmetry, movements, abnormalities.
B. Palpation
Using sense of touch
Assess: texture, temperature, moisture, size, consistency, tenderness.
C. Percussion
Tapping to produce sounds
Determine: organ size, density, borders; detect fluid/air.
D. Auscultation
Listening to body sounds
Assess: heart, lung, and bowel sounds with stethoscope.
Visual aid showing systematic examination sequence. Alt text: Diagram illustrating head-to-toe physical examination approach with PILCODD components highlighted.
🩺 Clinical Tips & Important Notes
Communication Tips
- Always introduce yourself and explain the process
- Use open-ended questions initially (“Tell me about your pain”)
- Maintain eye contact (culturally appropriate)
- Summarize and confirm your understanding
Examination Essentials
- Wash hands before and after examination
- Ensure adequate lighting and privacy
- Compare symmetrical body parts
- Proceed from least to most intrusive examinations
Documentation
- Record findings immediately
- Use patient’s own words for chief complaint
- Note negative findings when relevant
- Maintain confidentiality always
Quick Knowledge Check
Question: Which component of history taking includes information about tobacco, alcohol, and occupation?
Topic Tags
Physical Examination
PILCODD
LQQOPAAA
Inspection
Palpation
Percussion
Auscultation
Chief Complaint
HPI
Medical History
Clinical Skills
Diagnosis
Patient Assessment
General Medicine
First Aid
CTEVT
Health Assistant
Clinical Examination
Systemic Examination
📋 Summary & Key Points
- History taking is primarily subjective; physical examination provides objective data
- PILCODD provides a systematic approach to general examination
- LQQOPAAA ensures comprehensive history of present illness
- The four core examination techniques are: Inspection, Palpation, Percussion, Auscultation
- Always maintain patient dignity, privacy, and confidentiality
- Effective communication builds trust and improves diagnostic accuracy
- Documentation should be accurate, timely, and use standardized terminology
For further reading, visit the CTEVT official website or consult standard medical textbooks like Bates’ Guide to Physical Examination.
📥 Download Notes
Get a printable PDF version of these notes for offline study or reference. HA Basic Medical Procedure Unit 1 History taking and physical examination Notes
Includes all content, mnemonics, and summary tables. HA Basic Medical Procedure Unit 1 History taking and physical examination Notes